Techniques of Mandibular Anesthesia including Inferior Alveoar Nerve Block

Mandibular Anesthesia
Lower success rate than Maxillary anesthesia (approx. 80-85 %)Related to bone density
Less access to nerve trunks
Mandibular Nerve Blocks Inferior alveolar
Mental - Incisive
Buccal
Lingual
Gow-Gates
Akinosi
Mandibular Anesthesia Most commonly performed technique
Has highest failure rate (15-20%)
Success depends on depositing solution within 1 mm of nerve trunk
Inferior Alveolar Nerve Block
Not a complete mandibular nerve block.
Requires supplemental buccal nerve block
May require infiltration of incisors or mesial root of first molar
Nerves anesthetized
Inferior Alveolar
Mental
Incisive
Lingual
Body of mandible, inferior ramus
Buccal mucosa anterior to mental foramen
Anterior 2/3 tongue & floor of mouth
Lingual soft tissue and periosteum
Buccal anterior soft tissue
Lingual anesthesia
Patients at risk for self injury (eg. children)
10%-15% positive aspiration
Incisive nerve block
Anterior infiltration
Periodontal ligament injection (PDL)
Gow-Gates
Akinosi
Intraseptal
Mental
Incisive
Lingual
Areas Anesthetized
Mandibular teeth to midline Body of mandible, inferior ramus
Buccal mucosa anterior to mental foramen
Anterior 2/3 tongue & floor of mouth
Lingual soft tissue and periosteum
Indications of inferior Alveolar nerve block
Multiple mandibular teethBuccal anterior soft tissue
Lingual anesthesia
Contraindications of inferior Alveolar nerve block
Infection/inflammation at injection sitePatients at risk for self injury (eg. children)
10%-15% positive aspiration
Alternatives for inferior Alveolar nerve block
Mental nerve blockIncisive nerve block
Anterior infiltration
Periodontal ligament injection (PDL)
Gow-Gates
Akinosi
Intraseptal
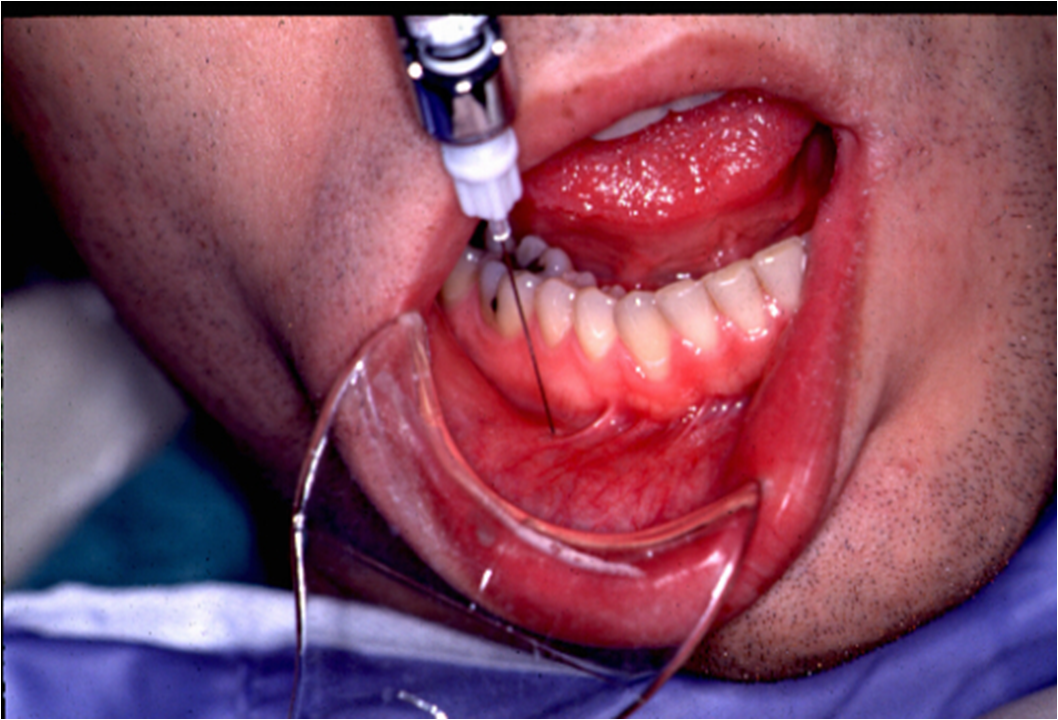
Technique for of inferior Alveolar nerve block
Apply topical anaesthesia
Area of insertion:
Medial ramus, mid-coronoid notch, {kind=link}
Level with occlusal plane (1 cm above),
3/4 posterior from coronoid notch to pterygomandibular raphe
Advance to bone (20-25 mm)




Target Area
Inferior alveolar nerve, near mandibular foramen
Landmarks
Coronoid notch
Pterygomandibular raphe
Occlusal plane of mandibular posteriors
Inferior Alveolar Nerve Block
PrecautionsDo not inject if bone not contacted
Occlusal plane of mandibular posteriors
Inferior Alveolar Nerve Block
PrecautionsDo not inject if bone not contacted
Avoid forceful bone contact
Failure of Anesthesia in inferior Alveolar nerve block
Injection too low
Injection too anterior
Accessory innervation
Mylohyoid nerve
Contra lateral Incisive nerve innervation
Trismus
Facial paralysis
Provides buccal soft tissue anesthesia adjacent to mandibular molars
Not required for most restorative procedures
Buccal Nerve Block
Indications
Anesthesia required - mucoperiosteum buccal to mandibular molars
Contraindications
Infection/inflammation at injection site
Advantages
Technically easy
Contra lateral Incisive nerve innervation
Complications of inferior Alveolar nerve block
HematomaTrismus
Facial paralysis
Mandibular nerve block Other Techniques of Manidilar nerve block
Long Buccal Nerve Block
Anterior branch of Mandibular nerve (V3)Provides buccal soft tissue anesthesia adjacent to mandibular molars
Not required for most restorative procedures
Buccal Nerve Block
Indications
Anesthesia required - mucoperiosteum buccal to mandibular molars
Contraindications
Infection/inflammation at injection site
Advantages
Technically easy
High success rate
Disadvantages
Discomfort
Discomfort
Alternatives
Buccal infiltration
Gow-Gates
PDL
Intraseptal


Insertion distal and buccal to last molar
Target - Long Buccal nerve as it passes anterior border of ramus
Insert approx. 2 mm, aspirate
Inject 0.3 ml of solution, slowly
25-27 gauge needle
Area of insertion:- Mucosa adjacent to most distal
Intraseptal


Technique
Apply topicalInsertion distal and buccal to last molar
Target - Long Buccal nerve as it passes anterior border of ramus
Insert approx. 2 mm, aspirate
Inject 0.3 ml of solution, slowly
25-27 gauge needle
Area of insertion:- Mucosa adjacent to most distal
Landmarks
Mandibular molarMucobuccal foldComplications
Hematoma (unusual)
Positive aspiration-0.7 %
Provides sensory innervation to buccal soft tissue anterior to mental foramen, lip and chin
Contraindication
Infection/inflammation at injection site
Advantages
Easy, high success rate
Mental Nerve Block
Terminal branch of IAN as it exits mental foramenProvides sensory innervation to buccal soft tissue anterior to mental foramen, lip and chin
Indication
Need for anesthesia in innervated area
Infection/inflammation at injection site
Advantages
Easy, high success rate
Usually atraumatic
Disadvantage
Hematoma
Alternatives
Local infiltration
PDL
Intraseptal
Inferior alveolar nerve block


Complications
Hematoma
Positive aspiration-5.7 %
Originates in mental foramen and proceeds anteriorly
Good for bilateral anterior anesthesia
Not effective for anterior lingual anesthesia
Nerves anesthetized
Inferior alveolar nerve block
Gow Gates

Complications
Hematoma
Positive aspiration-5.7 %
Incisive Nerve Block
Terminal branch of IANOriginates in mental foramen and proceeds anteriorly
Good for bilateral anterior anesthesia
Not effective for anterior lingual anesthesia
Nerves anesthetized
Incisive
Mental
Areas Anesthetized
Mandibular labial mucous membranes
Lower lip / skin of chin
Incisor, cuspid and bicuspid teeth




Indication
Anesthesia of pulp or tissue required anterior to mental foramen
Contraindication
Infection/inflammation at injection site
Advantages
High success rate
Infection/inflammation at injection site
Advantages
High success rate
Pulpal anesthesia w/o lingual anesthesia
Disadvantages
Lack of lingual or midline anesthesia
Lack of lingual or midline anesthesia
Complications
Hematoma
Positive aspiration-5.7 %
GOA PUBLIC SERVICE COMMISSION
EDC House, Block ‘C’, 1st Floor,
Dada Vaidya Road, Panaji-Goa 403001.
The last date for receipt of applications in the office of the Commission is03.05.2012. Casa J.D. Fernandes Stationery Supplier, Printers & Book Binders, Opposite Municipal Garden, Panaji, are authorized to sell the prescribed application form @ Rs. 20/- per set.
DENTAL COLLEGE & HOSPITAL
Lecturer in Public Health Dentistry ..… 2 Posts (1 resvd. for OBC)
Scale of pay: Rs. 15,600-39,100+5,400/-
Age: Not exceeding 40 years.
Educational & Other Qualifications:-
Essential: (i) A qualification included in Part I or Part II of the Scheduleto the Dentists Act, 1948 (16 of 1948).
(ii) Post-Graduate qualification in Dentistry i.e.
Master of Dental Surgery in concerned speciality/subject from a recognized Institution or equivalent.
(iii) Should be registered with Dental Council.
(iv) Three years experience as Registrar/Tutor/Senior Resident/Demonstrator in the concerned Speciality of Dentistry in a recognized Dental College /Medical College with Dental Wing/Dental Institution.
(v) Knowledge of Konkani.
Desirable: (i) One year teaching experience after post graduation in a recognized institute.
Hematoma
Positive aspiration-5.7 %
2 MDS required by Goa Public Service Commision
GOA PUBLIC SERVICE COMMISSION
EDC House, Block ‘C’, 1st Floor,
Dada Vaidya Road, Panaji-Goa 403001.
The last date for receipt of applications in the office of the Commission is03.05.2012. Casa J.D. Fernandes Stationery Supplier, Printers & Book Binders, Opposite Municipal Garden, Panaji, are authorized to sell the prescribed application form @ Rs. 20/- per set.
DENTAL COLLEGE & HOSPITAL
Lecturer in Public Health Dentistry ..… 2 Posts (1 resvd. for OBC)
Scale of pay: Rs. 15,600-39,100+5,400/-
Age: Not exceeding 40 years.
Educational & Other Qualifications:-
Essential: (i) A qualification included in Part I or Part II of the Scheduleto the Dentists Act, 1948 (16 of 1948).
(ii) Post-Graduate qualification in Dentistry i.e.
Master of Dental Surgery in concerned speciality/subject from a recognized Institution or equivalent.
(iii) Should be registered with Dental Council.
(iv) Three years experience as Registrar/Tutor/Senior Resident/Demonstrator in the concerned Speciality of Dentistry in a recognized Dental College /Medical College with Dental Wing/Dental Institution.
(v) Knowledge of Konkani.
Desirable: (i) One year teaching experience after post graduation in a recognized institute.
(ii) Knowledge of Marathi
For Full and Correct information please visit :http://nicgoa.nic.in/gpsc/ad_file.php
For Full and Correct information please visit :http://nicgoa.nic.in/gpsc/ad_file.php
Some Amazing Dental facts your Dentist didn’t tell you
By : Dr GAURAV ARORA.....
Dental health is quite intriguing. There are plenty of myths around that we blindly believe and follow. Dental health is a whole science in itself and there is a lot more to it than appears so. Here are some interesting facts that an average person does not know about dental health.
The commonly used practice of putting a cap on toothbrush is actually more detrimental. The moisture entrapped in the cap favors bacterial growth.
You are not supposed to brush within 6 feet of a toilet. The airborne particles from the flush can travel up to a distance of 6 feet.
People who tend to drink 3 or more glasses of soda/pop daily have 62% more tooth decay, fillings and tooth loss than others.
The first toothbrush with bristles was manufactured in China in 1498. Bristles from hogs, horses and badgers were used. The first commercial toothbrush was made in 1938.
Fluoridated toothpastes when ingested habitually by kids can lead to fluoride toxicity.
You are supposed to replace your toothbrush after you have an episode of flu, cold or other viral infections.
Notorious microbes can implant themselves on the toothbrush bristles leading to re-infection.
New born babies do not have tooth decay bacteria. Often, the bacteria are transmitted from mother to baby when she kisses the child or blows in hot food/drink before feeding the baby.
Lecture by Dr. Bruno Tedesco on MTA splinting & Post Core on
Saturday 5th May ...
Venue : Hotel Amara
SCO - 137, sector-43 B
chandigarh
Fee : Rs. 500 ( Free material worth 350 with cocktail & Dinner.)
For registrations : Call Paramjeet ( 9815328103 begin_of_the_skype_highlighting 9815328103 end_of_the_skype_highlighting )
What is the proper technique for tooth brushing?
Because every mouth is different, there is more than one technique of brushing that has proven to be effective. Deciding which technique is most appropriate for you depends largely on your teeth position and gum condition etc.Faulty tooth brushing can harm your teeth by wearing off the protective enamel layer, causing hypersensitivity and bleeding from the gums.
Consult your dentist to determine which technique is most appropriate for your mouth.
Generally, most dentists recommend the Modified Bass method for adults. This method cleans most effectively in areas where gum infections start first and is easy to master.
Step 1: Take a pea-sized amount of toothpaste onto a soft brush.
Step 2: Tap the brush to allow the paste to sink in deeper.
Step 3: Place it into the mouth, starting from the last 3 teeth in the arch. The bristles of the brush should be at 45 degrees angulation facing the gumline, placed partly on the gums and partly on the teeth.
Step 4: With slight pressure being applied, give 18-20 vibratory strokes. This dislodges and loosens all debris from the tooth surface.
Step 5: Now give a sweep towards the chewing surface. Then shift to next three teeth overlapping one tooth of the previous three teeth covered. Change the toothbrush at least once every three months, or when the bristles appear frayed.
Why is flossing important?
Brushing alone cannot remove plaque that is located in places that a toothbrush cannot reach-particularly between teeth. In addition to removing plaque, flossing also helps to:
Remove debris that adheres to teeth and gums in between teeth.
Polish tooth surfaces.
Control bad breath.
Join dis group of facebook for JObs & vacancies related to Dentistry...
http://www.facebook.com/groups/faithdental/
Regards
Dr.Gaurav Arora